Michael Moore’s film, Sicko, dramatically illustrated how problems in access to health care in the United States have escalated to the point of a crisis for all but the richest Americans. The problems include the fact that many citizens are uninsured, health care costs are increasing faster than inflation and wages, and more of those costs are being passed on from employers to employees. Many indices of health care effectiveness show that the United States fares very poorly in comparison to other developed capitalist countries. Almost all the other developed capitalist countries have universal health care. All their citizens are insured and their per capita costs are much lower.
The crisis will get airtime before the 2008 presidential elections, despite the Republican candidates shying away from it. But the solutions offered by leading Democrats, if ever enacted, will prolong the crisis. Clinton and Edwards want to mandate citizens’ coverage, with subsidies and tax credits for those who cannot afford it at all. The costs would be enormous, the inequalities mildly tweaked, and the profits of the insurance and drug companies barely touched. Obama deals with it through employers, not even addressing the unemployed. Insurers will still fight tooth and nail against all three, because all three plans would forbid them to deny coverage based on pre-existing conditions.1 The issue is fertile ground for consciousness-raising education, since it affects all of us, and really digging out from under the crisis will reveal how the U.S. class structure promotes profits instead of basic rights such as health care. This article will review several dimensions of the crisis. Proposals to ameliorate the situation will be discussed, including their limitations, as well as opportunities that the debate offers for advancing a progressive agenda.
1. Dimensions of the Crisis
The Problem of the Uninsured and Rising Costs
Sicko vividly portrays the plight of people denied benefits by insurance companies. But 47 million Americans—16 percent—have no health insurance at all,2 about 20 million are underinsured, and 108 million have no dental insurance.3 Families that have insurance via an employment-based health plan contribute an average of $3,281 a year.4 The employee share of health insurance premiums rose from 14.0 percent in 1992 to 22.1 percent in 2005, not including the higher deductibles or copays paid by employees that also have occurred over this same time period.5 Health insurance costs have been increasing three times as fast as wages.6 Chart 1 illustrates this. However, the ratio of private industry employer spending on health care, including insurance, to profits has been cut in half between 1986 and 2005.7
Chart 1: Cumulative changes in health insurance premiums, overall inflation, and workers’ earnings, 2000–06
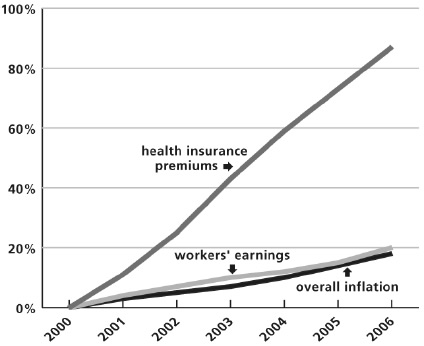
Note: Data on premium increases reflect the cost of health insurance premiums for a family of four.
Source: KFF/HRET, “Survey of Employer Sponsored Health Benefits, 2001–2006,” http://www.kff.org; Bureau of Labor Statistics, “Customer Price Index, U.S. City Average of Annual Inflation (April to April), 2001–2006,” http://www.bls.gov.
Not only has the percentage of people covered by employer-based health care been decreasing. The percentage covered by government-provided health care has also been decreasing. In addition, among working-age adults who shopped for health insurance on their own over the last three years, 89 percent were rejected for health reasons or found it too expensive.8 Fewer and fewer Americans can afford to get well.
This is in the context of an overall deterioration of the economic well being of the working class. Wages and salaries now make up the smallest share of the nation’s gross domestic product since the government began recording the data in 1947, while corporate profits have climbed to their highest share since the 1960s.9 The value of worker’s benefits no longer keeps pace with inflation. The median hourly wage declined 2 percent since 2003, after adjusting for inflation, even though productivity—the amount that an average worker produces in an hour—has risen steadily over the same period. In fact, wages have declined since 2000 while productivity has risen rapidly.10 Looking back even further, productivity has risen to the extent that in 1950 a worker produced as much in one forty-hour week as she or he produced in just eleven hours in 2004. Wages rose continually from 1950 only until 1973. Since then they have stagnated, except for the rise between 1996 and 2000, during the technology boom.
The Problem Is Not Just Rising Costs, But Who Pays and What For
Health care spending is currently 16 percent of the gross domestic product.11 It is projected to rise to 25 percent by 2030. In 2003, the United States spent $5,635 per person on health, more than twice the average within the Organisation for Economic Co-operation and Development (OECD), an association of developed capitalist countries.12 This was around ten times more than the lowest-spending countries within the OECD, Mexico and Turkey. These costs have doubled in the past seven years,13 and now the annual premium that a health insurer charges an employer for a health plan covering a family of four averages $12,106.14 You might say that the costs have been keeping profits down. But you would be wrong.
Certainly the bosses scream louder and louder about the costs, as GM yells when it lays off thousands and uses the over $1,500 in health premiums that it pays out for each car produced as a lever against the remaining workers.15 However, over the past forty years, adjusting for inflation, corporate profits per worker have doubled while workers’ wages are lower.16 Not only do workers contribute $3,281 of the annual family premium, but they also shoulder the costs of deductibles and out-of-pocket expenses, which are also rising. Premiums for family coverage have increased 78 percent since 2001, while wages have risen 19 percent and the cost of living has climbed 17 percent.17 2006 was the tenth straight year that medical cost growth outpaced wage growth. In 2005 the annual premiums for family coverage eclipsed the gross earnings for a full-time, minimum-wage worker ($10,712).18 The reality is that costs have been shifted more and more onto workers’ backs.
So what do we get for our money? We certainly get more problems. Health care expenditure is the major component of household consumption responsible for the increase in household net borrowing and even the foreign deficit.19 More than half of all bankruptcy filings are directly related to medical expenses.20 Every thirty seconds in the United States someone files for bankruptcy in the aftermath of a serious health problem.21
As for the benefits of this debt debacle, Americans get very little bang for their buck. Comparisons to other OECD countries are disastrous. The United States has one of the highest infant mortality rates in the OECD.22 If the U.S. rate were lowered, for example, to Canada’s, over 20,000 more babies would survive every year. U.S. life expectancy is twenty-second among the thirty OECD countries, forty-eighth among the top fifty countries in the world, tied with Denmark, where half as much is spent per capita and everyone is insured.23
Since the rate of growth of medical expenditures in the United States was exactly the median of all OECD countries from 1991 through 2001, the United States can be expected to continue to be the highest spender for quite a while.24 Much of the growth is due to higher drug costs. Brand-name drug prices in the United States rise over 6 percent a year.25 Most other OECD countries control spending by holding down drug prices. And the drug industry has for decades been the most profitable in this country. In addition, the administrative costs of health care in the United States are higher, because many OECD countries have government-administered health insurance while in the United States there are many private competing insurers. The profits of insurance companies and the relatively new entities called health care corporations have skyrocketed.
Why Is the Grass Greener on the Other Side of the Border?
Both the infant mortality and overall mortality rate in Canada are much lower than those of the United States. Life expectancy in Canada is more than two years longer. Yet annual per capita spending is close to $3,000 less there. The major difference between there and here is that Canada has a single-payer system. The government pays for almost all medical costs. In the United States there are many competing private insurance companies, some operating for profit and some not for profit. The profits amount to a fortune for the owners of the for-profit companies.
Both Canada and the United States are marked by inequalities such as those of class and race, as well as fairly rotten health habits, thus enabling meaningful comparisons between them. In 1970, the two countries had identical statistics regarding the relationship of inequality to mortality. That was the same year that Canada converted to single-payer, and the figures have never been the same since.26
Inequality in mortality rates is now rampant in the United States. For example, among the most destitute Americans, a 1 percent increase in income translates to a mortality decline of 22 fewer deaths in 100,000 people. There is no such relationship in Canada.27 The inequalities in U.S. health care exacerbate the already severe socioeconomic inequalities and injustices in the country. In higher-wage firms 67 percent of workers are covered by their own employer, compared to 47 percent of workers in lower-wage firms.28 While the overall U.S. life expectancy rate is 77 years, the rate for blacks is about 72 years with black males at a third-world level of 68 years.29 While high blood pressure, heart disease, and diabetes are rampant among the poor and working class, there are few programs to improve the income-related lifestyle. Insurance companies have begun to sponsor programs to promote healthier eating habits, exercise, and so forth, to limit their expenses for costly procedures and hospitalizations. However, insurers and individuals spend vast sums on medications that are palliatives which assure high profits for pharmaceutical companies. These drugs, like cholesterol-lowering statins, often under-perform lifestyle changes. In the United States, over $250 billion is spent annually on drugs, realizing a 15.7 percent profit for the drug industry, as a percentage of its revenues.30 From the pharmaceuticals’ point of view, public health is the opposite of wealth. In Canada, such a degree of exploitation is against the law.
2. Proposed Solutions
Is Single-Payer the Answer?
Would eliminating private health insurance plans and replacing the current chaos with a Canadian-style system paid for through payroll taxes help? Surely zeroing out insurance company profits and lowering the administrative costs that many competing plans entail would reap huge savings. Analyses of single-payer plans estimate that eliminating the current system would result in a one-time savings of 10 to 20 percent of costs, about $200 billion.31 According to Physicians for a National Health Program, just the potential savings on paperwork, more than $350 billion per year, are enough to provide comprehensive coverage to everyone without paying any more than we already do. And this is without the savings that containing drug costs would reap. Health care would be both affordable and universal, and the inequalities in health care would no longer contribute to the overall inequalities of U.S. society. So single-payer would be a big step in the right direction.
Medicare for All?
Single-payer is somewhat like Medicare for all, with health care provided primarily by private doctors and hospitals. Medicare, a universal health insurance program for older Americans, spends less than 2 cents of every dollar on administrative costs, and spends 98 cents on care.32 Private insurers spend 80 cents of each dollar on medical care and spend much of the other 20 cents on denying insurance to those who need it. But Medicare has problems.
Medicare is facing a disaster, not only from rising medical costs, including the insurance and drug company profits, but also due to the fact that millions of baby boomers will soon be added to the program that currently insures 42.5 million Americans. In ten years federal spending on Medicare is expected to be about double what it is now. The right wing would like to apply a wrecking ball to Medicare, as well as Social Security, and render them bygone memories of a social safety net. (The net has always been flimsy, and has suffered from increasingly enormous holes starting in the 1980s.) President Bush’s proposal to slash Medicare spending was part of the wrecking-ball approach, but it did not manage to get by the re-election concerns of members of Congress in 2006.
Private insurance companies have been dipping their paws into Medicare for quite some time. Then came the Medicare Modernization Act of 2003, written by drug and insurance company lobbyists, who then made sure that it passed in Congress.33 It includes a prescription drug benefit (Part D) for Medicare recipients but prevents Medicare and Medicaid from negotiating lower prices with drug companies and bars the importation of drugs from Canada. Drug and insurance companies are already raking in new profits from the law. For example, in 2007, drug companies will see a $2 billion dollar windfall that our taxes pay for.34 This is because the 2003 Medicare law mandated that 6.5 million low-income elderly people or younger disabled poor people be transferred from Medicaid into Part D of Medicare. The price that the drug companies charge for Medicaid enrollees are lower than those for Medicare, thus yielding the $2 billion for the drug makers. For insurance companies, their subsidies will be increased by $14 billion over ten years by the 2003 Medicare overhaul legislation.35
In addition, big Part D insurers like Wellpoint and UnitedHealth are using the drug plan to recruit members for Medicare Advantage, the managed care plans operated by private insurers but subsidized by Medicare. This is part of the increasing privatization of Medicare, whereby seniors buy private health insurance from companies that get subsidies from the government. In Medicare Advantage, there are HMO and PPO options, as well as private fee-for-service plans targeting seniors in Medigap, a supplemental policy that helps them pay for expenses that conventional Medicare does not cover. The government is paying the private insurance industry a subsidy of 11 percent per patient, on average, to provide fee-for-service plans. That amounts to the government paying private industry at least $770 million more than the government would spend covering those patients itself. Humana, for one, offers low premiums and copayments to attract customers to its drug plan, which is subsidized by Medicare at $75 per person per month. But Humana’s reward for luring a customer into a full Medicare Advantage policy is a government subsidy of $900 to $2,000 a month above whatever the patient pays.36 A health care securities analyst at Citigroup says that by expanding Medicare-subsidized offerings, the insurance industry has a potential revenue opportunity of more than $450 billion a year, or enough to almost double the revenue of the managed care industry.37
If single-payer were to be the universal health care plan adopted, and if it were truly like Medicare for all, in the privatized direction that Medicare is currently going, it would be another welfare program for capitalists. But the version of single-payer (H.R. 676) proposed by Representative Conyers, is different.38 It would come close to eliminating the private insurers’ roles, insure everyone, contain medical costs (including negotiating lower drug prices), and save both private industry and the public billions in its first year.
Is it Socialized Medicine?
The California legislature recently passed a single-payer plan that would have reduced total health care payments in the first year, insured everyone currently uninsured (six million Californians), protected consumers’ ability to choose their own doctors, and allowed the state to negotiate bulk rates for prescription drugs and medical equipment. Governor Schwartzenegger vetoed the bill, lying about the costs and calling it “socialized medicine.”
Backers claim that H.R. 676 will institute a nonprofit health care system. That is only partially true. It is a move in the direction of socialized medicine, since it nearly eliminates insurance companies and also cuts drug company profits. In a minor concession to free enterprise, it also retains privately administered care by doctors, hospitals, and other providers.
Here is an example of completely socialized medicine: When I was in Cuba in 1978 I took a friend to a clinic for a digestive ailment. She was treated immediately and successfully with no appointment, no lines, free medicine, and no bills. Of course in Cuba no insurance or drug companies parasitically make profits from health care. Sicko provides similar but recent illustrations. And poor little socialized Cuba has a considerably lower infant mortality rate than the United States.39
Beneath the lies and name calling, Schwartzenegger and the capitalists he represents—insurance and drug companies in this instance—have real reasons to oppose H.R. 676. Single-payer would almost eliminate insurance companies, copayments, and premiums. Controlling drug costs would mean that pharmaceutical companies, ballooned by profits from monopolizing patents and exploiting publicly funded research, would have to dream up new con games. The United States spends over $250 billion a year on drugs. Without government patent monopolies, the cost would be $70 billion.40 So single-payer would hit profits hard, even if it is not quite socialism.
What About Other Plans?
In contrast to California, Massachusetts (with Governor Romney’s support) recently passed a universal plan that has no cost controls but makes it a finable offense for anyone not to have health insurance. The plan subsidizes people who earn up to 300 percent of the poverty level, but since a typical group policy in Massachusetts costs more than $11,000 for family coverage, many families are forced to choose between complying with the law and other vital necessities. If such criminalization of the uninsured worked, it would be a windfall for insurance companies and at this point, it appears to be having that exact result. As of December 1, 2007, only 37 percent of the 657,000 uninsured had gained coverage under the new program, but 79 percent of these newly insured individuals are very poor people who had been enrolled in Medicaid or similar plans and were eligible for completely free care funded by the state. Now they face copayments under the new plan. Moreover, the subsidies mean that public funds for the care of the poor that previously flowed directly to hospitals and clinics now flow through insurance companies with higher administrative costs.41
Punishing the uninsured is a central element in the “universal health care” proposals of both Edwards and Clinton. They are expensive and are nothing like socialized medicine. Obama’s proposal only requires employer contributions toward employees’ health plans and mandates that children be insured. However, all three are the butts of the “socialized medicine” pejorative because they compel insurance companies to accept applicants regardless of pre-existing conditions and attempt to rein in premiums.
3. What We Are Up Against and the Implications
The Reaction
Capitalists who moan and groan about health care costs would find help in any universal plan. For years manufacturers like GM have spent more on health care than on steel, and retailers like Starbucks spend more money on health care than on coffee.42 Some capitalists, like Wilbur Ross, an investor in the steel and auto industries, realize that “Every country against which we compete has universal health care. That means we probably face a 15 percent cost disadvantage versus foreigners.”43 But in this age of interlocking directorates, manufacturers cannot just look out for their own narrow interests. For example, six of the eleven directors on GM’s board have or recently have had high positions in drug, insurance, or health care companies.44 The board protects those interests as well.
A single-payer plan would eliminate premiums for employers, which would be like a $600 billion a year tax break for them—the largest by far in history.45 So while single-payer would even benefit many capitalists, the prospect is irking to two of U.S. capitalism’s most powerful sectors. How powerful? The drug industry pays more than $100 million a year—and that is just at the federal level—for lobbying, while the health insurance industry pays over $30 million.46 The entire health industry lobby amounts to $400 million a year. The ante will surely be raised to defeat it if single-payer ever gets close to passage.
An Uphill Battle
Single-payer would be a first step toward parity with other developed capitalist countries, begin to dig this country out of this crisis, and help reveal how the class structure promotes profits instead of basic rights, such as health care. It is the only “universal health plan” that works economically, since its savings come from insurance company profits and administrative costs as well as drug company profits. Demanding its passage can be an organizing and educational tool that promotes a socialistic vision of how things could work. It has captured the imagination of enough people that it might even win in some local battles.
Single-payer will not win nationally as an isolated issue. The power and financial resources of the insurance and drug industries are likely to defeat even the proposals of the most mealy-mouthed of presidential candidates if they threaten one dollar of insurance and drug profits. Even if one of these recent proposals were to pass without compromise, it would be so costly and misguided that it would probably collapse from its own shortcomings. But the role of profit and the reaction of profiteers can be used by a wider movement that brings to the fore broader issues that include the demand that health care be a right, not a privilege. For that movement to have breadth and strength it must put forth clearly what a socialist vision brings to health care and other social issues, as well as the shortcomings of compromises that are proposed by politicians from capitalist parties.
Notes
- Ezra Klein, “Candidates Go Code Blue on Healthcare,” Los Angeles Times, September 30, 2007, http://www.latimes.com.
- U.S. Census Bureau, “Health Insurance Coverage: 2006,” http://www.census.gov.
- Carole Fleck, “Nothing to Smile About,” AARP Bulletin, September, 2006.
- Molly Selvin and Daniel Costello, “Workers Paying More for Coverage,” Los Angeles Times, September 12, 2007, http://www.latimes.com.
- Lawrence Mishel, “Employers Shift Health Insurance Costs onto Workers,” http://www.epi.org.
- Matthew Benjamin and Kerry Young, “Americans Without Health Benefits May Have Set Record (Update 1),” August 29, 2006, http://www.bloomberg.com.
- Employee Benefit Research Institute, Databook on Employee Benefits, Chapter 34, 2006, http://www.ebri.org.
- Lisa Girion, “Study Says Individual Insurance Too Costly,” Los Angeles Times, September 14, 2006.
- Steven Greenhouse and David Leonhardt, “Real Wages Fail to Match a Rise in Productivity, New York Times, August 8, 2006, http://www.nytimes.com.
- Lawrence Mishel, Jared Berstein, and Sylvia A. Allegretto, “The State of Working America 2006/2007,” Economic Policy Institute, http://www.stateofworkingamerica.org.
- Joshua Holland, “Two Trillion Spent on Healthcare Each Year,” Alternet, July 28, 2007, http://www.alternet.org.
- OECD, “Drug Spending in OECD Countries Up by Nearly a Third Since 1998, according to New OECD Data,” http://www.oecd.org.
- David Leonhardt, “The Choice: A Longer Life or More Stuff,” New York Times, September 26, 2006, http://www.nytimes.com.
- Selvin and Costello, “Workers Paying More for Coverage.”
- Leonard Wiener, “The Big Benefit Squeeze,” U.S. News and World Report, March 13, 2005, http://www.usnews.com.
- U.S. Government Printing Office, “Economic Report of the President: 2005 Report Spreadsheet Tables,” http://www.gpoaccess.gov.
- Selvin and Costello, “Workers Paying More for Coverage.”
- Guy T. Saperstein, “Medicare for All: The Only Sound Solution to our Healthcare Crisis,” Alternet, January 16, 2007, http://www.alternet.org.
- Nelson H. Barbosa-Filho, Codrina Rada, Lance Taylor, and Luca Zamparelli, “US Macro Imbalances: Trends, Cycles, and Policy Implications,” Schwartz Center for Economic Policy Analysis, December, 2005, http://www.newschool.edu.
- David U. Himmelstein, Elizabeth Warren, Deborah Thorne, and Steffie Woolhandler, “MarketWatch: Illness And Injury As Contributors To Bankruptcy,” Health Affairs, February 2,2005, http://content.healthaffairs.org.
- Elizabeth Warren, “Sick and Broke,” Washington Post, February 9, 2005, http://www.washingtonpost.com.
- Lawrence Mishel, Jared Berstein, and Sylvia A. Allegretto, “The State of Working America 2006/2007,” Economic Policy Institute, http://www.stateofworkingamerica.org.
- OECD, “Health at a Glance—OECD Indicators 2005,” http://www.oecd.org.
- Victor R. Fuchs, “Health Care Expenditures Reexamined,” Annals of Internal Medicine (2005): 143:76–78.
- David Gross, Leigh Gross Purvis and Stephen W. Schondelmeyer, “Prescription Drugs: Trends in Manufacturer Prices of Prescription Drugs Used by Older Americans,” http://www.aarp.org.
- Holly Dressel, “Has Canada Got the Cure?” Yes Magazine, Fall 2006, http://www.yesmagazine.org.
- Holly Dressel, “Has Canada Got the Cure?”
- The Kaiser Family Foundation, “Employer Health Benefits: 2006 Summary of Findings,” http://www.kff.org.
- Merrill Goozner, “Time for a Checkup,” TomPaine.commonsense, September 21, 2004, http://www.tompaine.com.
- San Jose Mercury News, “Pelosi Courageously Takes on Powerful Lobby,” Editorial, December 15, 2006.
- Merrill Goozner, “Governor Terminates Single Payer,” Huffington Post, September 6, 2006, http://www.huffingtonpost.com.
- Paul Krugman, “Insurance Horror Stories,” New York Times, September 22, 2006, http://select.nytimes.com.
- Milt Freudenheim, “A Benefit for Insurers,” New York Times, March 31, 2006, http://www.nytimes.com.
- Milt Freudenheim, “A Windfall from Shifts to Medicare,” New York Times, July 18, 2006, http://www.nytimes.com.
- Freudenheim, “A Benefit for Insurers.”
- Freudenheim, “A Benefit for Insurers.”
- Freudenheim, “A Benefit for Insurers.”
- Marilyn Clement, “Single Payer Candidates Taking the Lead,” Portside,” August 25, 2006, http://lists.portside.org.
- Library of Congress, Federal Research Division, http://lcweb2.loc.gov.
- Dean Baker, “Prescription Drug Scams,” Truthout, June 29, 2006, http://www.truthout.org.
- Ed Kent, “An Open Letter to the Nation from Massachusetts Physicians: Early Outcomes from Massachusetts’ Health Care Reform,” Blogger News Network, January 3, 2008, http://www.bloggernews.net.
- Joe Nocera, “Resolving to Reimagine Health Costs,” New York Times, November 18, 2006, http://select.nytimes.com.
- Malcolm Gladwell, “The Risk Pool,” The New Yorker, August 28, 2006, http://www.newyorker.com.
- http://www.gm.com.
- Goozner, “Governor Terminates Single Payer.”
- M. Asif Ismail, “Drug Lobby Second to None,” The Center for Public Integrity, July 7, 2005, http://www.publicintegrity.org.
Comments are closed.